





Actor Lisa Ray’s revelation that chemotherapy induced early menopause at the age of 37 has sparked a vital conversation on an often-overlooked aspect of cancer treatment. Diagnosed with multiple myeloma in 2009, Ray spoke about the emotional and physical challenges of losing fertility and experiencing menopause unexpectedly, highlighting a gap in survivorship care.
Medical experts explain that chemotherapy, while targeting rapidly dividing cancer cells, can also damage ovarian cells, reduce egg reserves, and in some cases trigger temporary or permanent menopause. Women over 35–40, those undergoing longer treatment durations, or receiving certain drugs like alkylating agents are at higher risk.
Fortunately, protective strategies exist if discussed early. Fertility preservation options include egg or embryo freezing, ovarian tissue freezing, and the use of GnRH analogues to temporarily suppress ovarian function during chemotherapy. In cases where pelvic radiation is planned, ovarian transposition may also be considered. While no method guarantees prevention, early planning significantly improves outcomes.
Chemotherapy-induced menopause, often called “chemopause,” remains under-discussed. During diagnosis, the primary focus is survival, and reproductive or hormonal concerns may feel secondary. Social stigma around discussing reproductive health further contributes to the lack of awareness.
Hormone replacement therapy (HRT) can alleviate menopausal symptoms and protect bone and cardiovascular health but must be individualized. In hormone-sensitive cancers, HRT is generally avoided, while survivors without hormone-driven cancers may consider it under medical guidance.
Ray’s candid disclosure underscores that surviving cancer involves more than treatment success. Informed discussions about fertility, symptom management, and long-term hormonal health are essential for improving the quality of life for women undergoing chemotherapy.

ରାଜଧାନୀ ଦିଲ୍ଲୀର ଜନ୍ତର ମନ୍ତରରେ ଚାଲିଥିବା ଛାତ୍ର ଆନ୍ଦୋ...
ବଲାଙ୍ଗିର ଜିଲ୍ଲାର ଲୋୟର ସୁକତେଲ ପ୍ରକଳ୍ପକୁ ନେଇ ମଙ୍ଗଳବା...

ଓଡ଼ିଶାକୁ ମିଳିଛି ଆଉ ଏକ ବଡ଼ ଶିଳ୍ପ ପ୍ରକଳ୍ପ। କେନ୍ଦ୍ର ସ...
APAAR (Automated Permanent Academic Account Regist...
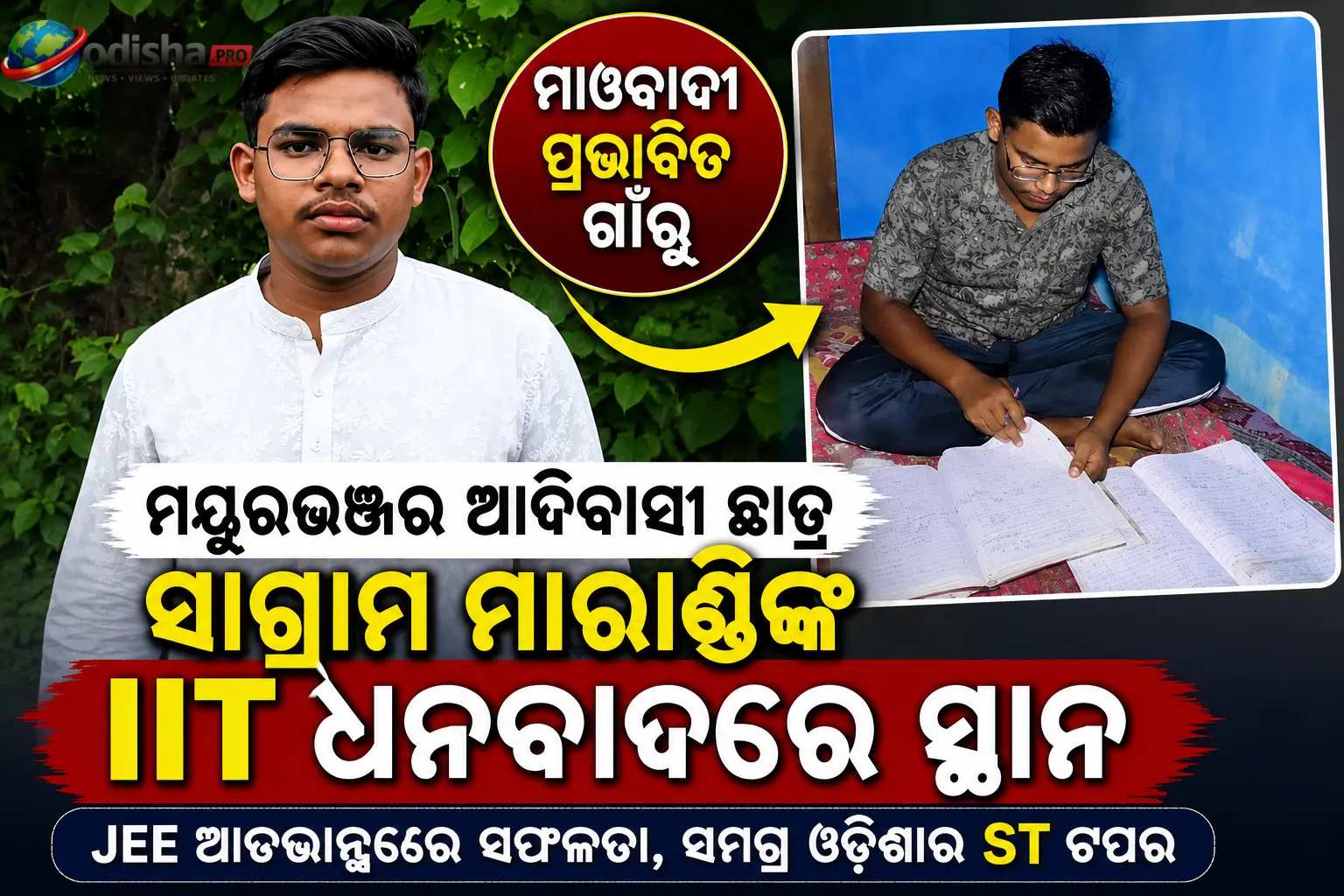
ମାଓବାଦୀ ପ୍ରଭାବିତ ଅଞ୍ଚଳରୁ ଆସିଥିବା ଜଣେ ଆଦିବାସୀ ଛାତ୍ର...
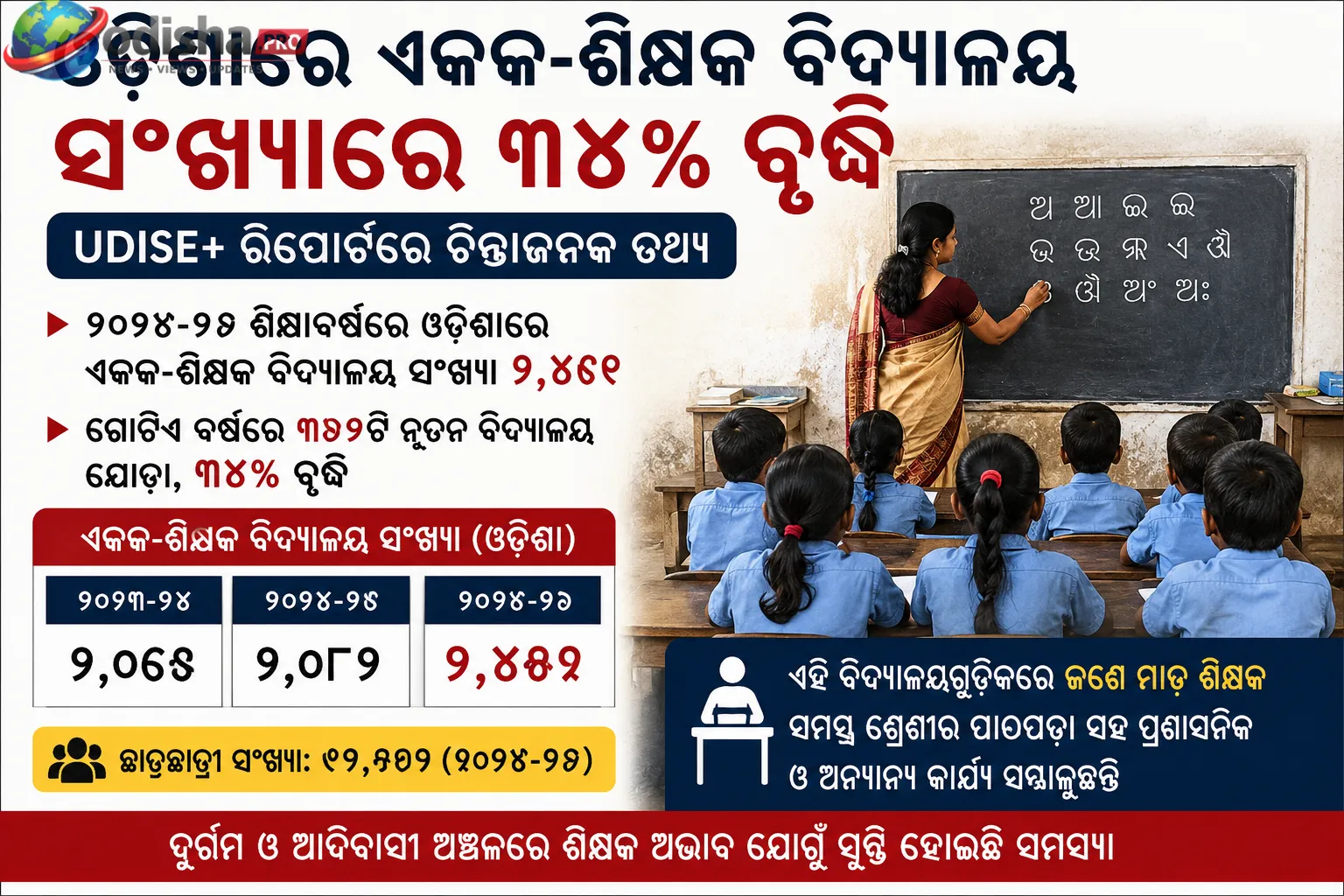
୨୦୨୫-୨୬ ଶିକ୍ଷାବର୍ଷରେ ଓଡ଼ିଶାର ଏକକ-ଶିକ୍ଷକ ବିଦ୍ୟାଳୟ (...

ଅଦାନୀ ଗ୍ରୁପ୍‌ର ଅଦାନୀ ଏନର୍ଜି ସଲ୍ୟୁସନ୍ସ ଲିମିଟେଡ...
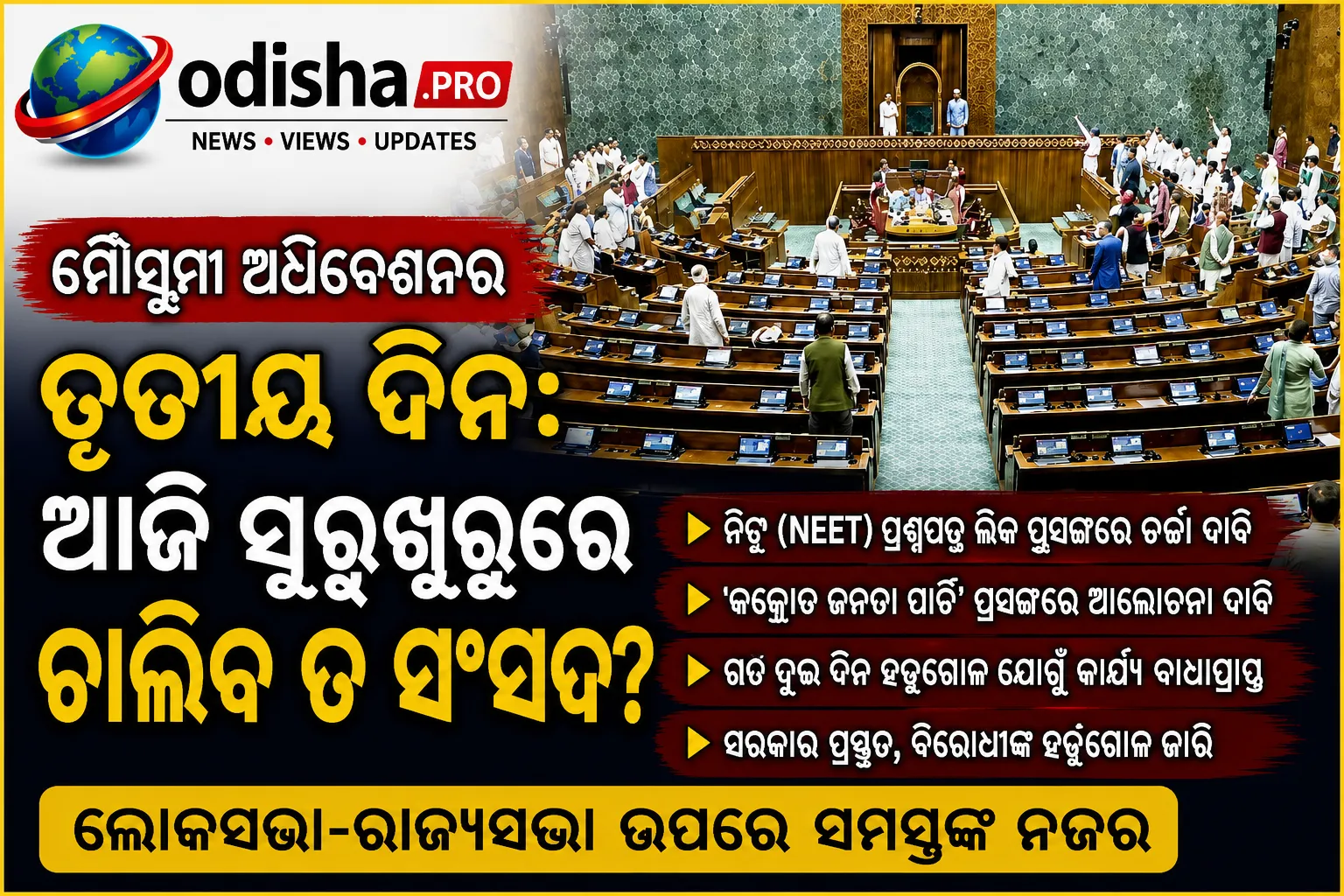
ସଂସଦର ମୌସୁମୀ ଅଧିବେଶନର ଆଜି ତୃତୀୟ ଦିନ। ଗତ ଦୁଇ ଦିନ ଧର...
SCERT ପାଠ୍ୟପୁସ୍ତକରେ ତ୍ରୁଟି ଘଟଣାକୁ ନେଇ ଚାଲିଥିବା କ୍ର...

ଦିଲ୍ଲୀର ଜନ୍ତର ମନ୍ତରରେ **‘କୋକରୋଚ୍ ଜନତା ପାର୍ଟି...

ସାଗରମାଳା କାର୍ଯ୍ୟକ୍ରମ ଅଧୀନରେ ଓଡ଼ିଶା ଦେଶର ଅଗ୍ରଣୀ ରାଜ...

ସଂସଦର ମୌସୁମୀ ଅଧିବେଶନର ତୃତୀୟ ଦିନ ବୁଧବାର ବିରୋଧୀ ସାଂସ...
